Private Equity, UnitedHealth Take a Huge Loss as Oregon Bans Corporate Control of Doctors
Oregon passes SB 951, a bill that prohibits private equity and corporate decision-making in health care. UnitedHealth Group, Amazon, and private equity lobbied fiercely, but lost. Is it a trend?
Welcome to BIG, a newsletter on the politics of monopoly power. If you’d like to sign up to receive issues over email, you can do so here.
Two days ago, Oregon Governor Tina Kotek signed the nation’s strictest law against corporate control of health care practices in the state. It’s a major defeat for private equity and large health insurers, and something that advocates and physicians have been advocating for years, as more and more of the state’s capacity got bought up by financiers. It’s also a ground-breaking event that could catalyze the creation of a new health care system, one managed by medical professionals and patients instead of Wall Street. And it’s all thanks to UnitedHealth Group.

In this piece, I’m going to walk through the politics of corporate power and private equity in health care and why it’s so hard to tackle, even though it’s such an obviously bad thing. And then I’ll explain why Oregon became the first state to actually go after the problem, and go after it hard.
The logic of the bill is clear. As Oregon nurses noted in lobbying for the bill, corporate control of medicine is fundamentally antagonistic to quality care, as it removes decision-making from medical professionals and patients and puts it in the hands of financiers. For instance, private equity owned clinics charge 20% more for the same procedures. Such ownership arrangements increase costs, make patient outcomes worse, and foster physician burnout, and of course, there are no improvements to quality or access.
We’ve known about this problem for awhile, and every few months a new book comes out pointing out that Wall Street institutional control of medical practices and hospitals costs us lives and money. And yet, there’s been little progress. So why did Oregon act? Why didn’t private equity and UnitedHealth Group’s lobbying succeed in this small Western state, when it has everywhere else? Well, part of the story is that it did succeed; in 2024, they were able to ward off this same law, which nearly passed but was not able to overcome fierce objections from state Republicans. But this year, something changed.
And we can actually thank UnitedHealth Group, which provided Oregon with a particularly noxious experience in health care, and the political culture to do something about it. Because UHG’s tactics are so brazen and extensive the company actually screwed over two separate Oregon state representatives, both of whom have cancer, and both of whom in turn testified on behalf of the bill. To understand how UHG messed up so badly politically, it helps to look at the actual process of how the bill got passed.
In March of 2024, Optum, the largest for-profit medical provider in America and a unit of UnitedHealth Group, applied for emergency approval to take over a large primary and specialty physician practice in Oregon, the 600 person Corvallis Clinic in Western Oregon. If the Oregon Health Authority didn’t approve the acquisition immediately, the clinic claimed, it wouldn’t be able to cover rent, payroll or other expenses. Only UHG’s cash infusion could keep the doors open. And this claim was likely true, Corvallis was in desperate financial condition.
What caused Corvallis’ cash crunch? Well, its application to Oregon regulators was redacted, but the American Prospect reported what insiders all knew - a different UHG subsidiary, the Change Health payment network, had been hacked and was nonfunctional, which meant that hospitals, pharmacies, and clinics nationwide couldn’t get paid for their services. And that included Corvallis Clinic, which couldn’t get access to money it was supposed to be paid by, among others, UnitedHealth Group. In other words, UHG caused a cash flow crisis at Corvallis, and then swooped in to buy it on the cheap.
Two months ago, Oregon state representative Sarah Finger McDonald gave testimony to the state legislature on what happened next. It’s an ugly story.
The most obvious impact was on the working conditions in the Corvallis clinic; doctors had to see too many patients, and began burning out. Nine primary care doctors left. Now the clinic isn’t accepting new patients. All of the neurologists departed as well, leaving entire counties without any of those specialists. Three of five gastroenterologists departed, and the two remaining ones no longer do on-call work. Medicaid insured patients can’t really use the clinic anymore, and Optum closed the lab for six months. These experiences affected not just Corvallis patients, but the entire region. They put pressure on other physician practices to accept an extra caseload, especially of poorer patients. Similarly, the other labs in the area are overloaded, and patients have to wait hours for a simple blood draw. McDonald herself has cancer, and she explained how she has “spent a lot of time” sitting around at the remaining regional lab.
The Corvallis acquisition was particularly notable because of the obvious bad faith in the acquisition, but it’s not unusual. In 2020, Optum bought the Oregon Medical Group, and since then dozens of doctors left. Earlier this year, however, thousands of potential patients were dropped, and insured patient costs have increased by twice the rate of state targets. One of those patients was state Rep. Lisa Fragala, who has breast cancer but then lost her doctor because of Optum’s cost-cutting. Here’s the headline that tells the broader story.

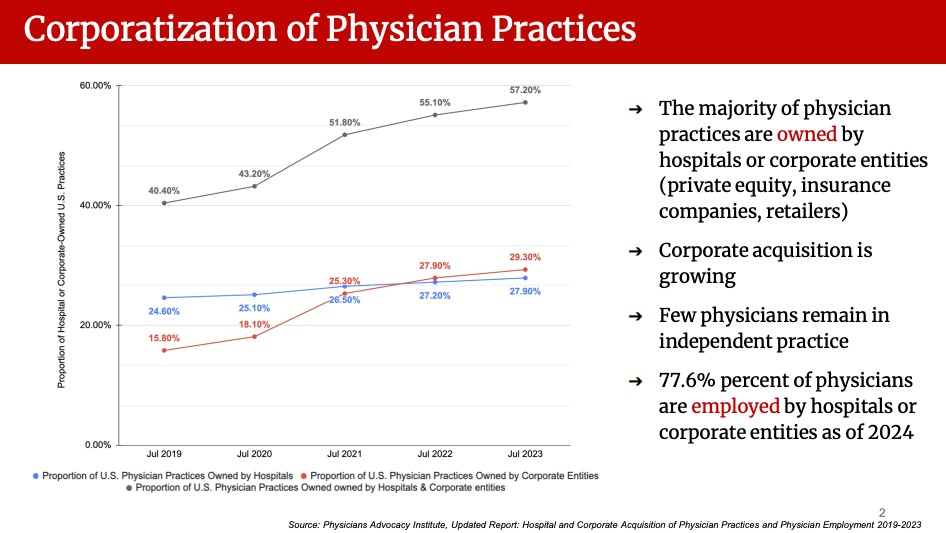
Dropping thousands of patients from quality care, including elected officials, generated real pushback. And Oregon is not unusual; nationwide, the practice of medicine is increasingly corporatized. Doctors just can’t hang out a shingle anymore, they lack the bargaining leverage as individuals to stay solvent in a land of paperwork giants.
What’s interesting about the problem of corporate control of medicine is that, in American history, it’s relatively new. Doctors and clinicians have always maintained as part of their professional practice, an approach to medicine that requires physician autonomy and respect for medical ethics. For more than a century, doctors sought to protect their autonomy by enacting laws that came to be known as “Corporate Practice of Medicine” statutes (CPOM). As Hayden Rooke-Ley and Erin C. Fuse Brown put it:
Dating back to the 1800s, CPOM laws generally bar unlicensed individuals and lay corporate entities from owning, employing, or controlling physicians and medical practices. These laws express a simple concept: An inherent tension exists between a physician’s ethical duty to patients and a corporation’s fiduciary duty to shareholders. In practice, however, CPOM bans have always had a less savory strain—they have been part of a larger regime of professional protectionism enforced by organized medicine, particularly the American Medical Association.
We shouldn’t overly romanticize the independent doctor in America, the doctor’s lobby opposed a host of important and useful public health measures, but it is true that the medical practitioner in America had the respect of being a local notable, and the legal protections it brought.
BIG is a reader-supported publication on monopoly and finance. If you are not yet a paid subscriber, please consider becoming one. We invest in finding out the truth. And yeah, that costs a few bucks, but in the long run it’s much cheaper.
In the 1970s, however, consistent with the rise of managed care, states began weakening CPOM laws, allowing hospital control of physician practices through a variety of corporate structures. Today, “management services organizations” (MSOs) often get around these laws by installing a friendly physician to serve as the face of the organization, seemingly complying with the CPOM laws. But the MSO sets hiring/firing policy, staffing levels, clinical standards, patient volume and visit length, and all key financial choices. They enact gag clauses and non-competes, locking in health professionals. That’s what happened in Oregon, which, though it has a CPOM law that says 51% of a practice must be owned by a licensed medical provider, has seen corporations take control of its clinical practices by using these tactics.
This new law is fairly simple; Oregon is simply closing up the loopholes that allow corporations to sidestep its CPOM rules. The law doesn’t block investment by corporations in medical practices, but it prohibits control of clinical practices by anyone but licensed medical providers. Now, a clinician, not a banker, must have decision-making authority over staffing levels, wait times, clinical decisions and operations, and as well diagnostic coding decisions, billing and collection policies, price setting, and payer contract negotiations.
The law also bans non-competes and gag clauses that lock in doctors and nurses, which was a major incentive for corporations to acquire practices and then worsen working conditions. It’s not ironclad; there are carve-outs for behavioral health, telehealth, and hospitals, and hospitals can still acquire clinical practices. iI’s also not immediate; It kicks into effect in three years, leaving substantial time to adjust, and it has a private right of action for enforcement, so aggrieved employees or competitors can litigate against lawbreakers. If you want the specifics, here’s the legislative analysisfrom the state Senate, and here’s a FAQ from Oregon Senator Deb Patterson, the main proponent of the bill.
The lobbying in the fight was aggressive, and not because Oregon is particularly important. The true fear is that this law could create a cascading effect in other states, who are considering or starting to limit the reach of private equity and large corporations in health care. Private equity, retailers like Amazon, and insurance conglomerates like Optum were telling state lawmakers that this bill would dry up capital to the medical industry. These groups acted as basically an open checkbook against passage of the bill. For instance, the Chamber of Progress, which is a tech association whose founder Adam Kovacevich was exposed by the Wall Street Journalas paying a respected antitrust expert, with a secret life as a sexual predator, to lie on behalf of Google in the early 2010s, lobbied against this Oregon CPOM bill. What does Chamber of Progress have to do with this legislation? Nothing. But the checkbook is open, so why not?

For the past forty years, whether HMOs, value-based care, or PBMs, the idea was that large vertically integrated corporations controlled by financiers would ration medical care and control physicians. Of course, to do that, corporate practice of medicine laws had to be defanged, and the judgment of independent pharmacists, nurses, doctors, and other clinicians subordinated to large corporations.
But over the course of the last five years, state and Federal lawmakers have begun hitting back at the broad corporatization of medicine across a host of areas, using traditional public utility tools of ownership restrictions, pricing regulations, and structural separations of lines of business where there are conflicts of interest.
This transformation is perhaps most advanced with pharmacy benefit managers, the large middlemen who have exerted control over pharmacists and pharmaceutical prices. The power of the big three PBMs, which are owned by some of the same corporations buying up clinical practices, is being neutralized. Arkansas just broke upUnitedHealth Group and CVS in the state, and Kentucky and Illinois are replacing giant PBMs with state-run pricing systems. There is even some PBM reform in the giant Federal GOP tax bill.
In physician practices and hospitals, there are also meaningful shifts; Pennsylvania, Massachusetts, and Minnesota have limited or are considering limiting hospital mergers. And Indiana, remarkably, is actually starting to engage in explicit price-setting in its hospital sector. This Oregon state law, by saying clinicians must be in control, instead of a transaction by transaction metric, is unusually important, because it is a straightforward rule about ownership and control, placing power of a socially valuable enterprise in the hands of the professional clinician running it. What’s exciting about the bevy of new laws is that we can see the seeds of a new health care system that replaces vertical integration and corporate control with rate regulation, transparency, and ownership rules based on ethical constraints.
All that said, there are limits to what this law can accomplish. Just banning certain forms of corporate control of certain medical practices isn’t sufficient to restore what’s been lost, or rebuild a patient and clinician centered medical system. The most powerful arguments against this bill are twofold. First, while the legislation does prohibit corporate control of clinical practices, it does not block hospital acquisitions of said practices, which is corporatization by another name. And second, a practice that can’t get sufficient reimbursements or financing, without anyone to sell to, will simply shut down.
These arguments against the bill, while legitimate, are just a recognition of how tilted against clinicians and patients our system really is. Ryan Grimm, President of the Oregon Ambulatory Surgery Center Association and an opponent of the bill, laid out his concerns in a letter. Grimm expressed fear that hospital acquisitions or closure might be the only exit for struggling clinics. He also noted that a lack of corporate money would mean that “clinics will not be able to acquire the very, very expensive multi-million dollar surgical equipment that is leading to revolutionary advances in patient care and patient outcomes.” Is that true? Well, probably not. Most corporate “investment” is about acquiring practices and eliminating capacity, not buying new fancy machines.
But there are a couple of important problems that have to be addressed. Large corporations can borrow money, and often do so cheaply, while clinical practices can’t. This dynamic is no different than the problem with homebuilders which Basel Musharbash wrote about a few weeks ago; the big builders can access bond markets, whereas the little ones no longer have banks to borrow from, which tips the market towards large firms with price-setting power.
We could see this dynamic playing out with the Optum acquisition of the Corvallis clinic in 2024. The clinic wrote, in its emergency application to be bought, that it was on the financial ropes, and was “unaware of any public or private source of capital that would be available to the Clinic to stabilize its operations” aside from UHG. It’s not just funding; big corporations and private equity groups can get supplies and medicine for cheaper than an individual or smaller practices, because of the pervasiveness of unlawful price discrimination in medical markets. And they can also get better reimbursement rates from payers because they have more bargaining power.
Ultimately, all of those problems must be fixed because they are all institutional reflections of a health system that is tilted against patients and clinicians, and towards financiers. We need public or bank-originated sources of capital for doctors and licensed medical providers to give them access to the same borrowing capacity as corporate entities, we need better reimbursement rates for smaller practices, and we need an end to price discrimination for pharmaceuticals and medical supplies.
I expect, now that this bill has passed, to see a “capital strike” against Oregon. Corporations like UnitedHealth Group will threaten and cajole, and otherwise tell lawmakers they will abandon or harm patients, more in sadness than anger, as they now have no choice. We may see high-profile announcements of closures, and lots of corporate friendly public relations in the form of articles saying that the Oregon law backfired, or that the big fancy lawyers are just so much more creative than public servants, and will find a way around these restrictions. Financiers always say they are winning, they say that if they are not allowed to win it’s bad for everyone, and they insist that everyone else is much stupider and will fail, so why resist in the first place? (Just eight months ago, Politico was reporting that “the momentum appears to have been stymied for now” to address private equity in health care.) Expect a deluge, a splattering, of pro-corporate arguments and tactics in Oregon, intended to frighten everyone back into the loving arms of UnitedHealth Group.
Hopefully, we’ll ignore that, and fix the problems that emerge. We will ideally see this law as one important step on a journey back to sanity, with follow-on laws providing capital and reasonable pricing/reimbursements to come, as well as more legal arrangements to move our corporate structured medical system towards one with a lot more pricing standardization and transparency. We already know that medical practices controlled by medical professionals do a much better job with patients, spending less on administrative bloat and pricing games and more on care. Ultimately, if clinicians have the same access to money and inputs as UnitedHealth Group or private equity, they will not only manage patients better, but they themselves will flourish.
Imagine that. Well, we don’t have to imagine, because Oregon just took a big step into that future.
Thanks for reading!
And please send me tips on weird monopolies, stories I’ve missed, or comments by clicking on the title of this newsletter. And if you liked this issue of BIG, you can sign up here for more issues, a newsletter on how to restore fair commerce, innovation and democracy. And consider becoming a paying subscriber to support this work, or if you are a paying subscriber, giving a gift subscription to a friend, colleague, or family member.
cheers,
Matt Stoller